Client Medication Worksheet
Description:
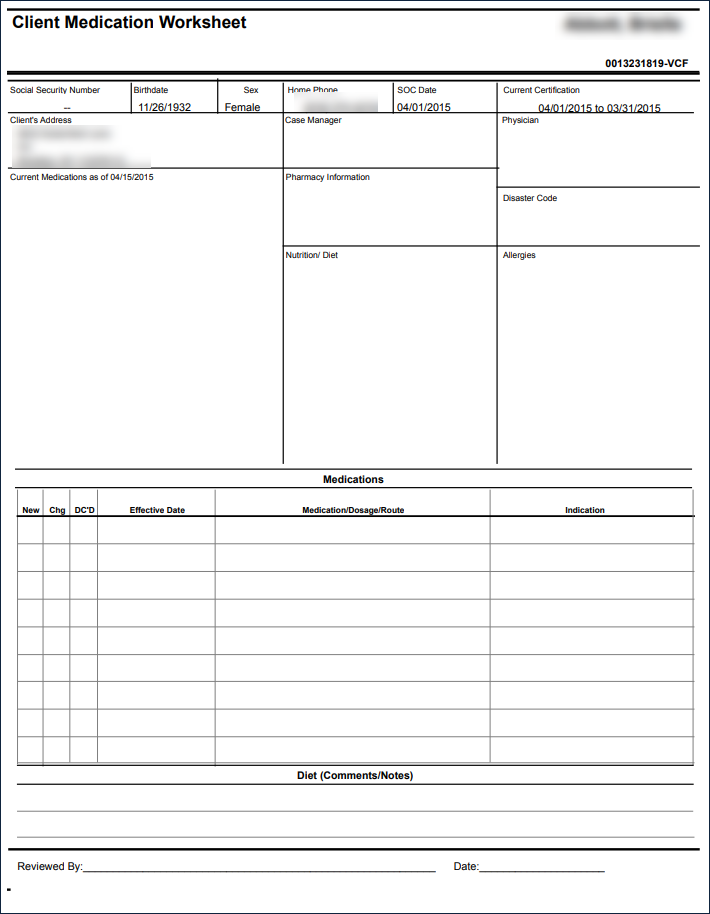
This report acts as a print-ready manual record of a client's medication information.
Use:
This report can be used by the agency to provide a physical copy of a medication sheet to either the client or a designated caregiver.
Limitations:
This report will not automatically populate most fields and is meant to be manually filled in after printing.
Filters
This report can be filtered by:
Field | Description |
|---|---|
Company | The selected company. |
Location | The selected location. |
Admit Type | The code for the client's admission. |
Team | The selected team. |
Client | Client by name (last name, first name) or Sandata Client ID. When a partial name is entered the report displays results that begin with the entered characters. |
Client Status | The selected client status. |
Date | The selected date. |
Report Output
Each column of the report displays:
Field | Description |
|---|---|
Client Name | The client's name (last, first). |
Chart ID | The client's Chart ID number. |
Social Security Number | The client's social security number. |
Birthdate | The client's date of birth. |
Sex | The client's designated sex. |
Home Phone | The client's home phone number. |
SOC Date | The client's start of care date. |
Current Certification | The client's current certification period. |
Client's Address | The client's primary address. |
Case Manager | The client's case manager. |
Physician | The client's primary physician. |
Current Medications As Of | The client's current medication. |
Pharmacy Information | The client's pharmacy information. |
Disaster Code | The client's disaster group. |
Nutrition/Diet | The client's nutrition/diet. |
Allergies | The client's allergies (if applicable). |
Medications | A table listing the client's medications. |
New | Indicates if the medication is new. |
Chg | Indicates if the medication has been changed. |
DC'D | Indicates if the medication has been discontinued. |
Effective Date | The date the medication is effective. |
Medication/Dosage/Route | The name, dosage, and route of administration of the medication. |
Indication | The condition that indicates the drug prescribed. |
Diet (Comments/Notes) | Written notes regarding the client's diet. |
Reviewed By | A signature field for the practitioner. |
Date | The date of the signature. |
Sample Report
Comments
0 comments
Please sign in to leave a comment.